
AI cannot decide if treatment was reasonable.
It can do something genuinely useful around that decision, though, and the difference is the whole point of this guide. Under section 16 of the Safety, Rehabilitation and Compensation Act 1988, a relevant authority pays compensation for the cost of medical treatment. But not automatically, and not for everything. The test is reasonableness, and reasonableness is a judgement. AI can build the picture you make that judgement on. It cannot make the judgement.
For a case manager, the section 16 medical treatment decision is one of the most frequent calls you make, and one of the easiest to rush. A treatment request lands, it relates to an accepted claim, the dollar figure looks ordinary, and it is tempting to wave it through. The statutory test asks more than that, and a structured AI work-up is a good way to make sure the more gets done every time. This guide gives you the test, two reusable prompts, a worked example, a Monday workflow and a pre-determination checklist to keep the whole thing inside the line.

What section 16 actually asks
Section 16(1) provides that where an employee suffers an injury, "Comcare is liable to pay, in respect of the cost of medical treatment obtained in relation to the injury (being treatment that it was reasonable for the employee to obtain in the circumstances), compensation of such amount as Comcare determines is appropriate to that medical treatment". For employees of licensees under the Act, the relevant authority stands in Comcare's place, and Comcare's guidance on the appropriate cost of medical treatment frames the provision exactly that way: once a claim is accepted, a relevant authority is liable to pay compensation of such amount as it determines is appropriate for treatment that was reasonably obtained. Read the subsection slowly, because it has three moving parts:
- the treatment was obtained in relation to the compensable injury, the accepted [CONDITION];
- it was reasonable for the employee to obtain in the circumstances; and
- the amount is appropriate to that medical treatment.
"Medical treatment" is itself a defined term. Section 4(1) lists the categories, and Comcare's guidance on the definition of medical treatment walks through them: medical or surgical treatment by or under the supervision of a medical practitioner, therapeutic treatment obtained at the direction of a medical practitioner, dental treatment, therapeutic treatment by or under the supervision of a registered physiotherapist, osteopath, masseur or chiropractor, examinations, tests and analyses requested by a practitioner and reports on them, the supply, replacement or repair of artificial limbs and other aids and appliances, treatment and maintenance as a patient at a hospital, nursing care and the provision of medicines and medical and surgical supplies, and any other form of treatment prescribed for the purposes of the definition. The first thing reasonableness needs is for the request to fall inside one of those categories. Something outside them is not section 16 medical treatment at all.
That category step is not a formality. Requests sometimes sit at the edge of the definition: domestic assistance, some home modifications, attendant care, or a gym membership framed as therapy. Whether a request falls within a section 4(1) category, or within a different head of compensation entirely, changes the test you are applying. Getting the category right first stops a reasonableness analysis being run against the wrong yardstick.
Comcare's guidance is explicit that reasonableness includes a cost-versus-benefit weighing. As its scheme guidance on applying the Clinical Framework puts it, "whether or not treatment is reasonable also involves a consideration of whether the cost of the treatment outweighs the benefits provided". The same guidance notes that the Administrative Review Tribunal has supported the use of the Clinical Framework as a relevant consideration in determining the reasonableness of medical treatment. The Clinical Framework for the Delivery of Health Services, published by WorkSafe Victoria, sets out five principles: measure and demonstrate the effectiveness of treatment, adopt a biopsychosocial approach, empower the injured person to manage their injury, implement goals focused on optimising function, participation and return to work, and base treatment on the best available research evidence. Those principles are not a checklist to pass or fail. They are the questions a reasonableness assessment should be able to answer, and a request that cannot speak to any of them is a request worth a closer look.
That is the test. Now here is where AI fits.
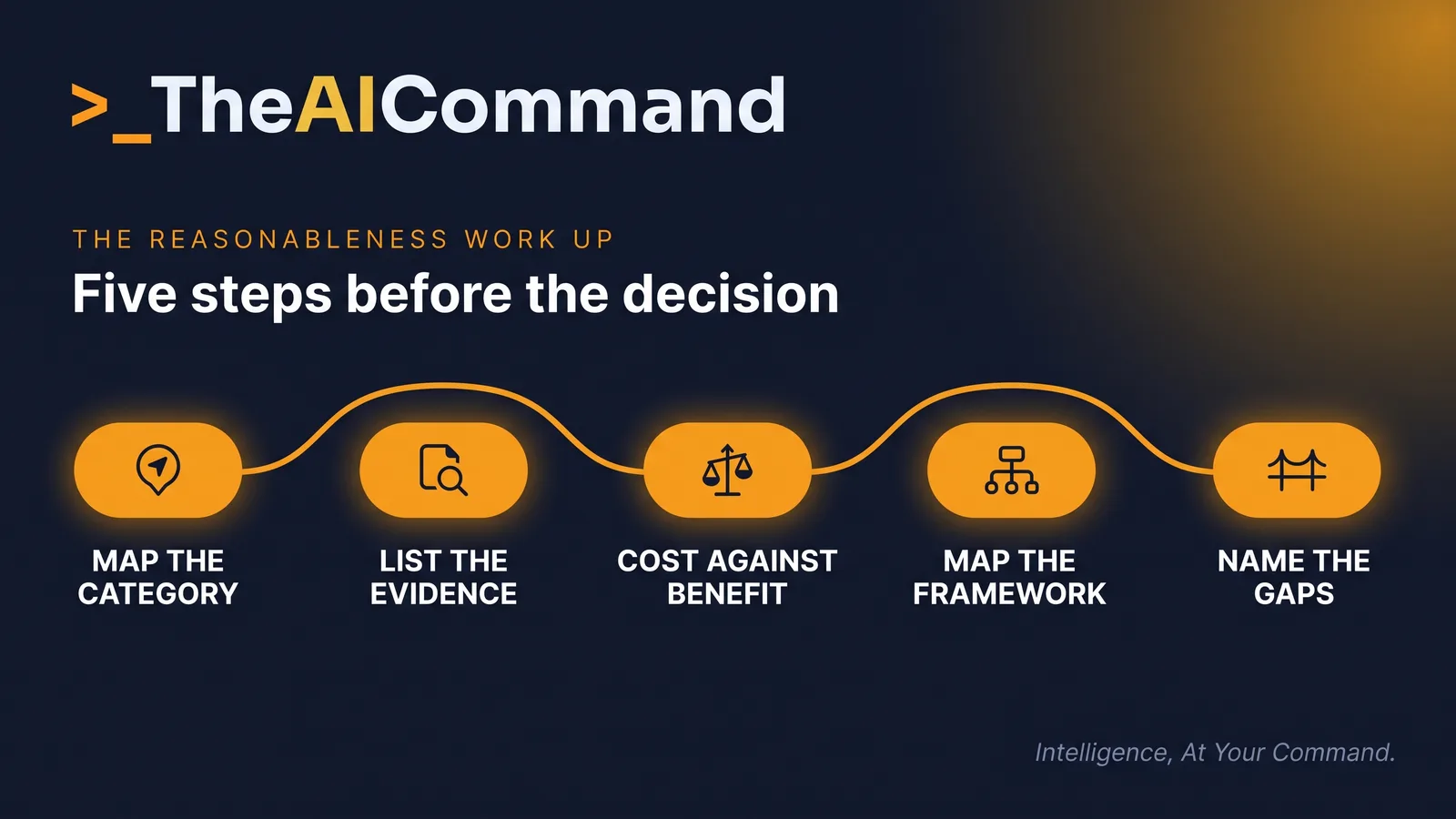
The AI reasonableness work-up
The job AI does well is assembly. A section 16 decision draws on a treatment request, the clinical rationale behind it, the accepted injury history, prior treatment and its results, and the cost. Those sit in different documents. Pulling them into one organised view is exactly the kind of work that eats a case manager's afternoon and that a model does in seconds.
Before any of this, de-identify. Strip the claimant's name, claim number, date of birth and any identifying detail before a single document goes near a general AI tool. Use placeholders: [CLAIMANTNAME], [CLAIMNUMBER], [CONDITION], [DATEOFINJURY]. If your organisation has not approved a tool for claim material, that approval comes first. Nothing in this guide overrides your privacy and information security obligations.
With a de-identified file, open your organisation's approved tool (ChatGPT, Claude or equivalent), paste this prompt, then paste the de-identified request and supporting documents beneath it.
The last instruction matters most. You are asking the model to organise and surface, not to decide. What comes back is a structured starting point: the category, the evidence, the cost and benefit summary, the Framework mapping and a gap list. You read it, you check it against the actual documents, and you make the call.
One thing the work-up should never do is invent the missing evidence. If the file does not contain a functional measure, the answer is to go and get one, not to ask the model to estimate it. A gap is a task for a person, usually a request back to the treating practitioner, not a prompt for the model to fill. The work-up is most valuable precisely because it names the gaps rather than papering over them.
Where the work-up earns its keep
The work-up matters most where the request is not obviously routine. A few patterns recur in section 16 decisions. An open-ended course of passive therapy with no measured improvement, where the cost keeps climbing and the functional benefit does not. A request for equipment or an aid where the question is whether it is reasonable for this injury rather than generally helpful. Treatment that sits outside the usual clinical pathway for the accepted [CONDITION], where the provider's justification carries all the weight. A spike in frequency or intensity without a corresponding change in the clinical picture.
In each of those, the reasonableness question is real and the evidence is scattered, which is exactly when a structured work-up beats a quick read. It will not tell you the answer. It will make sure you have seen the cost-versus-benefit picture, the Clinical Framework mismatch and the gaps before you decide, rather than after a reconsideration tells you what you missed.
Where AI helps and where it must not
AI helps with the parts that are mechanical. Finding the treating practitioner's stated rationale in a long report, building a treatment-and-outcomes chronology, flagging that the file says nothing about functional goals, noticing that the request does not obviously map to a defined category. These are organising tasks. A model is fast and tireless at them, and a tired case manager at four o'clock is neither.
AI must not do the weighing. Whether the cost outweighs the benefit, whether the treatment is reasonable in this person's circumstances, whether the clinical justification holds up, these are evaluative judgements the statute gives to the decision-maker. They are also the parts a model will confidently get wrong, because it will pattern-match to what usually happens rather than weigh what this file actually shows. The Clinical Framework assists the application of the test. It does not replace it, and neither does AI.
There is a hard line under all of this that has nothing to do with AI. A section 16 determination must be made by a properly delegated officer. A determination made by someone without the delegation is invalid, no matter how good the supporting work-up was. AI does not hold a delegation. It cannot make a determination, and a work-up it produced does not become a decision until a delegate applies the test and decides. Keep that sequence intact and the work-up stays a tool. Blur it, and you have an automated decision the Act does not permit.
A worked example, end to end
The situation. [CLAIMANTNAME], claim [CLAIMNUMBER], has an accepted [CONDITION] from [DATEOFINJURY]. A treatment request arrives for an extended course of hands-on therapy, well beyond the eighteen sessions already funded, supported by a short note from the provider asserting that the claimant continues to benefit.
The prompt used. The case manager de-identifies the request, the provider's note, the two most recent treatment summaries and the description of the accepted [CONDITION], then runs the work-up prompt above in the organisation's approved tool.
What came back. The request maps to therapeutic treatment under the section 4(1) definition. The provider's note asserts a benefit but does not measure one. The treatment summaries record no functional change across the funded sessions. There is no stated goal tied to function, participation or return to work. The cost is rising while the evidence of benefit is not. The gap list is specific: no current treating practitioner review, no functional measure, no stated goal, no expected duration or review point.
What the human verified and decided. The case manager rereads the provider's note and both treatment summaries against the model's summary, and checks the category mapping against the words of the section 4(1) definition. One error surfaces: the model described twelve funded sessions when the file records eighteen, a small slip that is exactly why the reread rule exists. The gaps are real, so the case manager drafts a request to the treating practitioner using the second prompt below, diarises the follow-up, and hands the completed picture, with the practitioner's response, to the delegated officer. The delegate weighs the evidence and determines the claim in deterministic language: compensation under section 16(1) is payable, or it is not payable because the evidence does not establish that the treatment was reasonable to obtain in the circumstances. Never "we feel" and never "it should be".
The model saved the assembly. The human caught the model's own error, closed the gaps and did the deciding. That is the pattern working as designed.
Your first work-up on Monday
- Pick one live treatment request that is not obviously routine: an extension of passive therapy, an aid or appliance, or anything outside the usual pathway for the accepted [CONDITION].
- Confirm which AI tool your organisation has approved for claim material. If none is approved, stop here and raise it. The rest of this workflow waits until that approval exists.
- De-identify the request and the supporting documents. Replace the name with [CLAIMANTNAME], the claim number with [CLAIMNUMBER], the date of birth with [DATEOFBIRTH] and every other identifying detail with a placeholder.
- Open the approved tool, paste the work-up prompt, then paste the de-identified documents beneath it and run it.
- Check the output against the source documents. Confirm the category mapping against the section 4(1) definition yourself, and reread every document the model summarised before relying on any summary.
- Action the gap list. Draft the request to the treating practitioner with the second prompt, review and send it, and diarise the follow-up.
- Hand the completed picture to the delegated officer, or, if you hold the delegation, apply the statutory test yourself and record your reasoning in your own words.
- Log the tool used, confirm on file that the material was de-identified, and record where the AI's involvement stopped.
The pre-determination checklist
Before any section 16 determination is made, the file should show:
- the request maps to a limb of the section 4(1) definition, checked by a person against the words of the definition;
- the treatment is linked to the accepted [CONDITION], not merely to the claimant;
- the treating practitioner's clinical justification has been located and reread in the source document;
- prior treatment and its measured outcomes sit in a chronology;
- the cost sits next to the expected benefit and the functional goal;
- the file has been mapped against the five Clinical Framework principles and the silences are named;
- every gap has been closed or requested, never estimated;
- everything that reached an AI tool was de-identified, and the tool is on the approved list;
- the tool used and the point where AI involvement stopped are recorded; and
- the decision-maker holds the delegation and has recorded their own reasoning.
For practitioners
Build the work-up prompt once and reuse it. Keep the instruction "do not reach a conclusion on reasonableness" in it permanently, so the tool stays an organiser. Always check the model's category mapping and its evidence summary against the source documents before you rely on either, because a confident summary of a document you have not reread is a trap. And run it only on de-identified material through an approved tool.
For governance leads
A reasonableness work-up is a defensible practice only if it is bounded. Set the boundary explicitly: AI organises section 16 evidence, delegated officers determine section 16 entitlements, and the two are never blurred. Require de-identification before any claim material reaches a model, restrict claims work to approved tools, log which tool was used, and make clear in policy that an AI work-up is an aid to the decision-maker, not a step in the determination. The audit question a governance lead should be able to answer is simple. For any section 16 decision, who held the delegation, what did they weigh, and where did the AI stop.
SRC Act sections referenced: section 16(1) (compensation in respect of medical expenses) and section 4(1) (definition of medical treatment).
Content disclaimer: This article is for general educational purposes only and does not constitute legal advice, liability determination guidance, or a substitute for professional judgement. Workers compensation decisions must be made by appropriately qualified and authorised persons under the Safety, Rehabilitation and Compensation Act 1988. All AI outputs described in this article require human review before use in any claims management context.
TheAICommand. Intelligence, At Your Command.


